




The sport will forever require its participants to push themselves psychologically, technically, tactically, and physically to succeed. It is this pursuit that captures the worlds attention over and over again. On the darker side of sport, an equally imposing phenomenon reaches its participants regardless of their level – Injuries. They have been occurring since sport began, and unfortunately, this trend isn’t leaving anytime soon. The incidence of injuries across many sports is always a topic of debate. Recently, there have been some longitudinal studies tracking the prevalence of soft tissue injuries across the world best teams in football. The studies indicate the incidence of injury hasn’t improved much over the last number of decades. This is despite the advances in technology, practises, number of staff etc. However, the demands of football have also increased significantly over that time. The games are more intense in terms of high-speed metrics; games are more frequent, players travel more often and attend more media events. This blog is not about debating whether or not things are improving in terms of injury in football. This is about using injury as a medium of learning and self-checking that what we are prescribing works. In my opinion, an injury leaves clues about an athlete’s biomechanical and physiological flaws. If we accept that injuries are just part of the process of playing a sport, we can miss valuable information about our athletes. The factors that contribute to injuries are well documented (previous injuries, sleep, training loads, etc). However, athletes still get injured if they had no previous injury, slept well, training load has been appropriate etc. This is the scenario I want the reader to imagine, and I would like to share my thoughts on this situation. Assuming all the other factors are not an issue like sleep or training load (which is what support staff/players are extremely good at ensuring), then why does an athlete breakdown?. I mentioned an injury leaves clue. I categorise these clues in three areas.

1st Clue – The Sport
This factor often gets overlooked, and too often, we treat athletes far too similar. The sport matters because the injuries matter. The injuries that occur in one sport does not mean they will appear across all. Every sport demands athletes to push themselves into various positions at varying speeds and/or forces that create energy throughout the body. The energy needs to be handled for athletes to be successful. That said, energy is expressed differently through a tennis player’s body than that of a footballer’s because the sport requires it. As a result, they experience different injuries throughout their careers. The sport identifies the array of possible injuries that could occur.
2nd Clue – The Mechanism
The mechanism behind an injury is very insightful and, if considered, can help with the rehabilitation, and prevent future injuries. The mechanism of an Anterior Cruciate Ligament injury will typically differ from that of a Posterior Cruciate Ligament. An injury mechanism is the coming together of forces, masses, momentum, gravity, AKA energy, that can expose a muscle, joint, connective tissue, etc. But as obvious as that sounds, the exact mechanism done twice can elicit two different injuries or no injury at all, which is why there is a third clue.
3rd Clue – The athlete or more precisely their biological & biomechanical make-up
This is a clue because if we take two footballers playing the same sport and experience the exact same mechanism, there is a chance that they could experience different injuries, or indeed, one may not get injured at all. To give an example would be two goalkeepers. One GK is hypermobile at the shoulder, meaning an excessive range of motion with a lack of stability. The other goalkeeper isn’t hypermobile at the shoulder and has good stability at end range. If they both attempt to save a hard strike in the top corner. The goalkeeper who is hypermobile is at more of risk of dislocating his shoulder versus the other. The sport (football) Sport Mechanism Athlete and mechanism (diving) could cause a dislocation because of his biological and biomechanical make-up. Hence, why our biomechanical and biological pre-dispositions can determine our injuries. We can expand this a little further to say it is the relationship between the mobility & the stability within and around a joint. This incorporates the inter and intra muscle coordination. We shall expand on this further in the blog.
To summarise, the sport indicates the type of injuries athletes are at risk of experiencing; the mechanism is the action that can expose the body to those injuries. And it is an athlete’s biomechanical and biological make-up that can determine the extent or type of injury.
There isn’t much we can do about the sport or even the mechanism, but there is undoubtedly a lot we can do about the biomechanics and biology of our athletes. Our method to affect this change is our exercise programme. However, not all exercises or training is equal. We have to purposely know what we are looking to change and check to see if that change is occurring than simply selecting exercises. Over the following few paragraphs and blogs, I will try to explain my thought process.

Let us talk about adductor injuries and, using the thought process above, meander our way through it.
1. 1st Clue – Sport
Groin pain is a frequent complaint in athletes. It occurs commonly in sports involving repeated sprinting, twisting, kicking and cutting such as soccer, rugby and Australian rules (Bradshaw and McCrory, 1997; Jansen et al., 2008b). Hip adductor muscle injuries are the second most common muscle injury in football (Ekstrand et al., 2011) and the most frequent acute groin injury in athletes (Serner et al., 2015). Adductor-related injuries constitute 64–69% of all groin injuries (Holmich, 2007) and 40% experience absence from football for more than 28 days (Holmich et al., 2014).
UEFA Elite Club Injury Study: 2017/18 season report
UEFA Elite Club Injury Study: 2018/19 season report
UEFA Elite Club Injury Study: 2019/20 season report
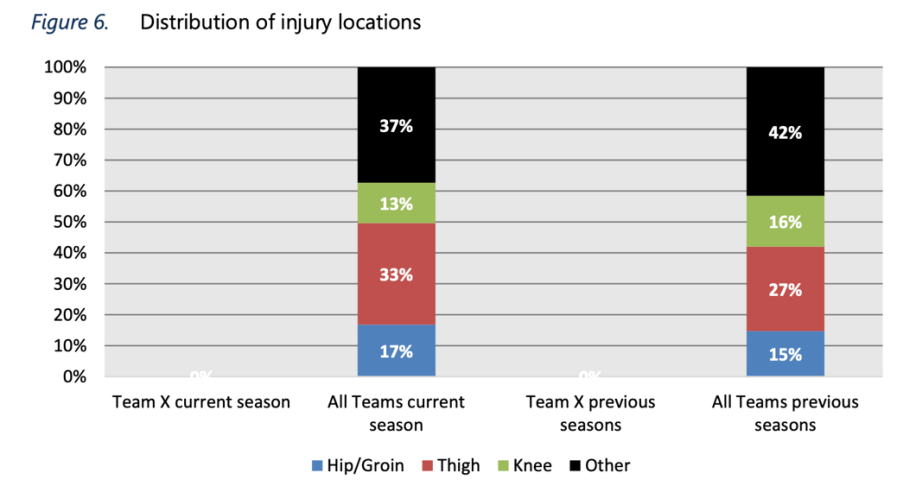
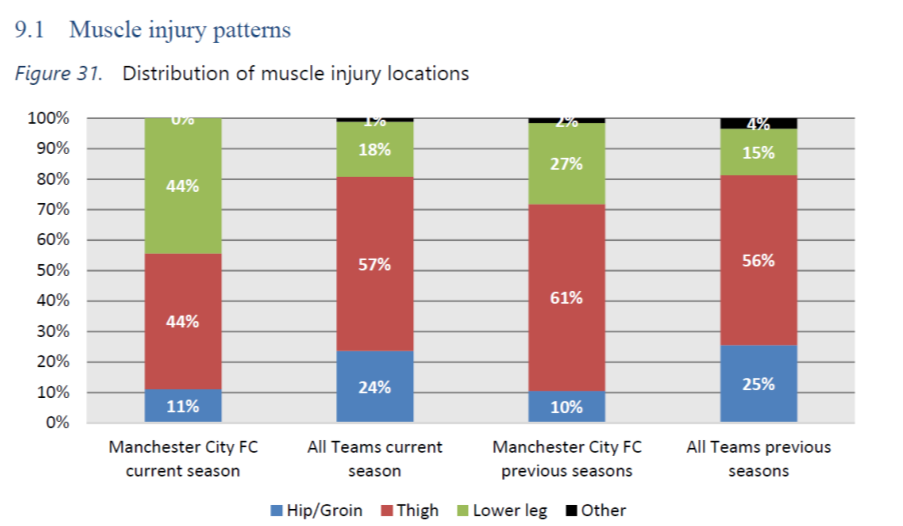
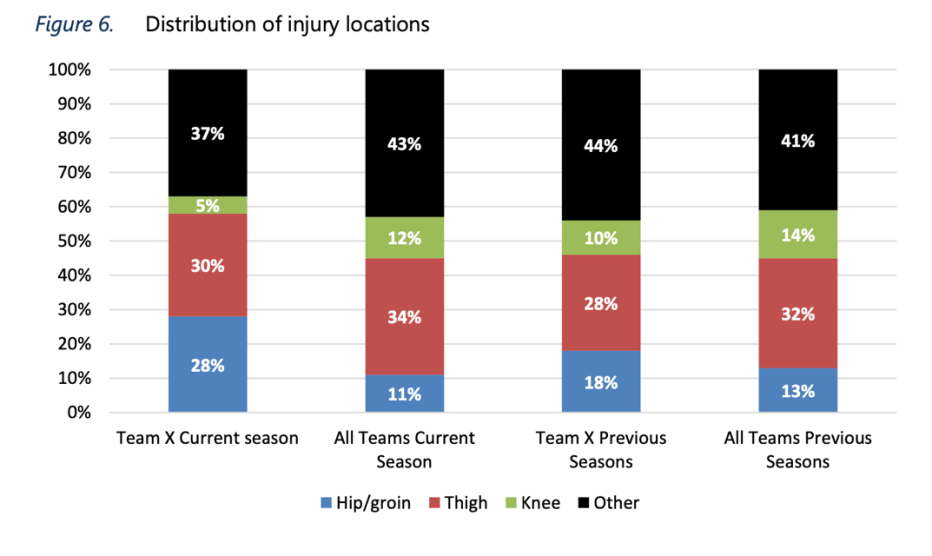
The UEFA elite injury study monitors the incidence of injuries across the world’s best football teams. The studies in the last three years have reported that hip/groin injuries account for 10%-28% of the injuries within those teams. It is evident that the demands of football can and will cause adductor injuries. The next thing to look at is the mechanism within the sport. What action in football causes players to get adductors issues?
Mechanism of Injury
When analysing injury incidence, understanding the mechanism is a necessary process to undertake. The process can help identify why it happened and how it happened and provides practitioners with some context for the rehabilitation process. Adductor injuries are relatively common, especially in football. The hip adductor muscles account for two-thirds of acute groin injuries in athletes, and the adductor longus is injured in 90% of these cases (Serner et al., 2015) Unfortunately, there isn’t an abundance of research on the injury mechanism for the adductors. However, one study investigated the mechanism of acute adductor longus injuries in football using systematic visual video analysis (Serner et al., 2018). They reported 4 different mechanisms for the 17 injuries investigated in their study.
The mechanisms reported were:
1. Change of direction (35%)
2. Kicking (29%)
3. Reaching (24%)
4. Jumping (12 %)
The authors reported that in the change of directions incidences, all injuries occurred at angles towards the side of the uninjured leg. Therefore, it was the trail leg that got injured. Of the reaching incidence, 3 out of the 4 injuries happened when the player reached for the ball with the uninjured leg. Similarly, the injury occurred in the trail leg. All the jumping incidences occurred as the player jumped off the uninjured side. Of the five kicking injuries, three were passes (two short, one long), and two were shots. Two were set plays (goal kick and penalty). Three were side-footed kicks and two in-step.
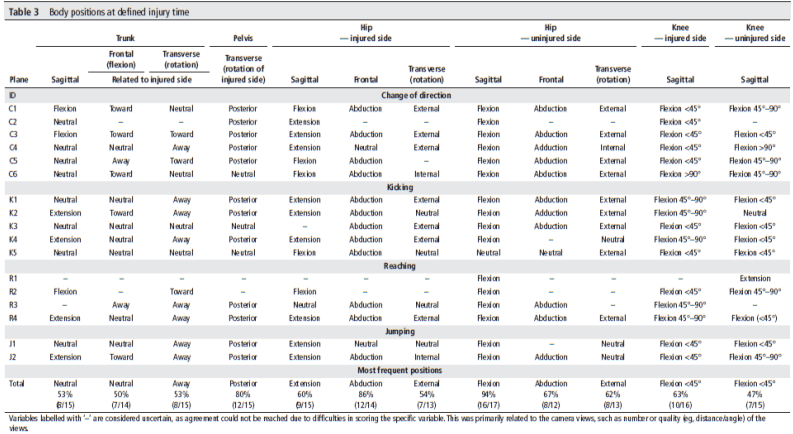
The above is a breakdown of the actions at the time of injury. Each incidence should be taken in isolation, but it is interesting when we analyse the loading pattern during the time of injury as an overview. For most incidences, the pelvis was going through posterior rotation (80%). In most of the incidences (53%), the trunk was rotating away from the injured side. This sequence will load the adductor longus proximally in the sagittal and transverse plane. It is difficult to note what is occurring in the frontal plane from the table above. In the hip, the most frequent positions involved extension and abduction, which would load the adductor longus in the frontal and sagittal plane. External rotation of the hip was also a regular position; this would, in fact, unload the adductor longus in the transverse plane. However, there could be instances where the femur was in external rotation but internally rotating, which would stress the adductor longus. Looking at instances of injuries as an average or trend isn’t best practice; however, if it only makes the point that muscles break down when they cannot cope with the demands or bone motions across all three planes, it is a worthwhile exercise.
We can’t avoid playing the sport, nor should we try. Consequently, the sport will generate mechanisms that cause injury, again something we cannot affect. So, the question is, how can we prepare our athletes to manage the sport and its mechanisms? In the next blog, we will dig deeper into this discussion.
References
Bradshaw, C. and McCrory, P. (1997) Obturator nerve entrapment. Clinical Journal of Sport Medicine, 7(3), pp. 217e9.
Ekstrand, J. and Hägglund, M. and Waldén, M. (2011) Epidemiology of muscle injuries in professional football (soccer), American Journal of Sports Medicine, 39, pp. 1226–32.
Engebretsen, A.H. and Myklebust, G. and Holme I, et al (2010). Intrinsic risk factors for groin injuries among male soccer players: a prospective cohort study. American journal of sports medicine, 38, pp. 2051–7.
Hölmich, P. (2007). Long-standing groin pain in sportspeople falls into three primary patterns, a “clinical entity” approach: a prospective study of 207 patients. British Journal of Sports Medicine, 41(4), pp. 247e52.
Jansen, J.A. and Mens, J.M. and Backx, F.J. and Stam, H.J. (2008b) Diagnostics in athletes with long-standing groin pain. Scandinavian Journal of Medicine and Science Sports, 18(6), pp. 679e90.
Serner, A. and Mosler, A.B, Tol, J.L and Bahr, R. and Weir, A. (2018) Mechanisms of acute adductor longus injuries in male football players: a systematic visual video analysis.British Journal of Sports Medicine, 0, pp. 1–8.
Serner, A. and Weir, A. and Tol, J.L. et al (2018) Characteristics of acute groin injuries in the adductor muscles: a detailed MRI study in athletes. Scandinavian Journal of Medicine and Science Sports, 28, pp. 667–76
Serner, A. and Jakobsen, M.D. and Andersen, L.L and Hölmich, P. and Sundstrup, E. and Kristian, T. and Serner, A. and Weir, A. and Tol, J.L. et al (2018) Characteristics of acute groin injuries in the adductor muscles: a detailed MRI study in athletes. Scandinavian Journal of Medicine and Science Sports, 28, pp. 667–76.
Werner, J. and Hägglund, M. and Waldén, M. et al (2009) UEFA injury study: a prospective study of hip and groin injuries in professional football over seven consecutive seasons. British Journal of Sports Medicine, 43, pp. 1036–40.

{kind=link}